
Follow all of PopSci’s COVID-19 coverage here, including the most recent numbers, tips on how to make your own masks, and advice on what to donate for health care workers.
In the midst of a crisis, everyone wants to know when it’s going to be over. That’s especially true right now, as many of us are sheltering in our homes to flatten the COVID-19 curve, and hoping things are at least moving in the right direction. So where are we in the course of this global pandemic?
The short answer is that we don’t—and can’t—know for sure. COVID-19 is unlike anything we’ve seen in the last 100 years, and given how much the world has changed since our last devastating upper respiratory pandemic, we can’t predict exactly how the disease will play out. But as researchers gather more and more data, they’ve started to be able to create models of how the novel coronavirus might spread and how big the impacts might be.
One such team at the Institute for Health Metrics and Evaluation came out with a new model this week that projects when the peak of the pandemic might hit each state, based on estimates of when we would need the most hospital and ICU beds. Their model incorporates the various social distancing measures implemented in each location thus far (and assumes that any states that haven’t already implemented the highest level of social distancing orders will do so within the next seven days). It assumes that these measures will be in place at least until the end of May.
Based on case count data released on April 2, their current model shows that the first wave could be over by early June. The top of the curve will likely occur around the second week of April, then run into May, though the disease will run its course differently in each state. At its peak, they estimate we’ll need 262,092 hospital beds and 39,727 ICU beds nationwide. Based on their data, that means we’ll be short more than 87,000 hospital beds and nearly 20,000 ICU beds. But the situation looks very different when you break out individual states.

A few states overshadow the rest, taking up the bulk of the total hospitalized patients. New York is by far the highest peak, with Alabama, California, Florida, Illinois, and Texas making up much of the rest.
It’s easier to get a sense of what might happen in any individual state by looking at each curve of cases on its own scale, so they don’t all pale in comparison to the population-dense New York.
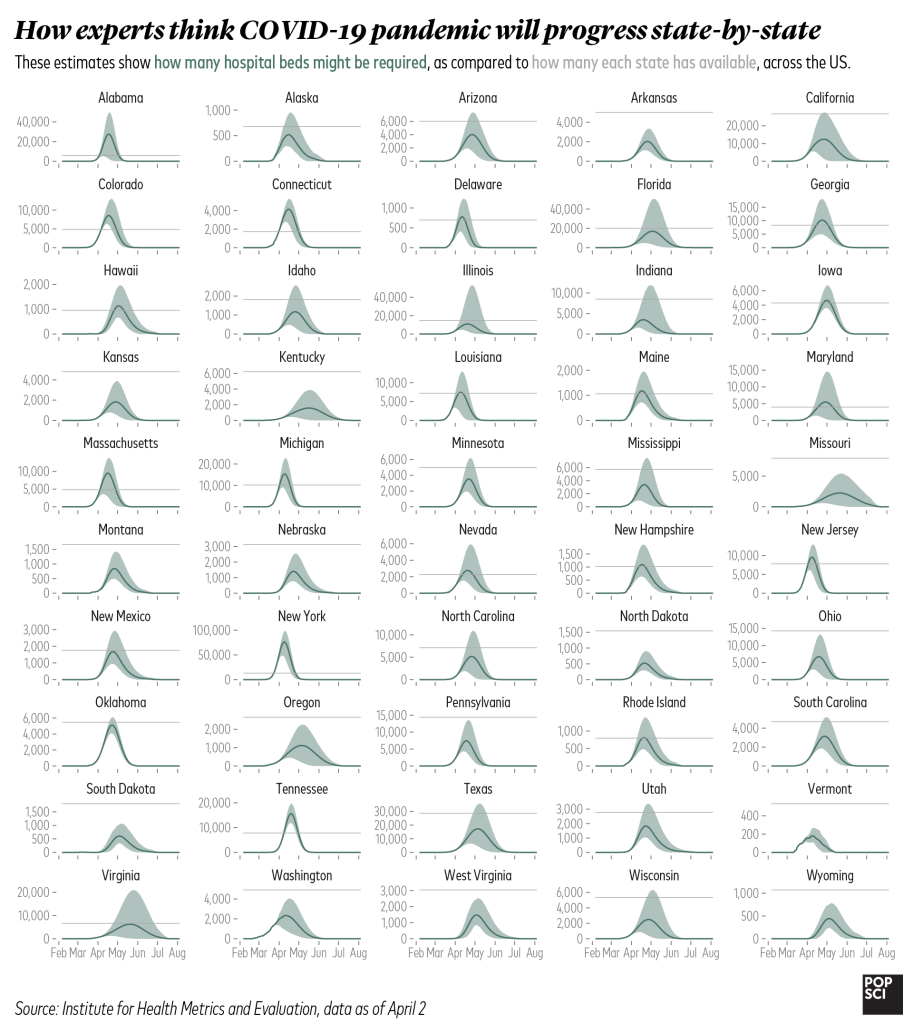
Here we can see just how many states are likely to exceed the number of hospital beds they have available. Even those with relatively low case numbers in absolute terms, like Connecticut, Nevada, and Maryland, are projected to run out of room. Some are in a grey area, where their totals might go over their available beds based on the current projection, but it’s still possible they might stay under capacity.
The peaks also vary in timing quite a bit. States hit early are likely to be on the downswing by May, while others will still be hitting their stride and ramping up new cases in the middle of that month.
The situation is even more dire for ICU beds. These are needed only for the sickest patients who are most likely to die, but most states are poised to be in short supply regardless of their overall case numbers.
Though the total numbers vary widely, we can see that most states are projected to exceed or meet their total number of available ICU beds. Many will be short by hundreds or thousands of beds. Shortages like this will mean that healthcare providers will be forced to take care of patients in suboptimal conditions and possibly to make difficult decisions about who gets life-saving care.
It’s also important to remember that when we talk about exceeding the number of hospital beds available, we’re not leaving any extra beds to treat people with conditions other than COVID-19. People don’t suddenly stop needing medical attention during a pandemic, and though stay at home orders mean fewer car accidents and other injuries, plenty of people without COVID-19 still need to be hospitalized, or even put in intensive care. If all of the beds need to be prioritized for those sick with the novel coronavirus, that leaves absolutely no room for folks with other ailments.
The IHME team estimate around 81,000 US deaths in total for this wave of the outbreak, though uncertainty in the model means it could be anywhere from roughly 38,000 to 162,000.
The important thing to remember is that these predictions aren’t perfect. As new data comes in, the outcomes can change, and our actions will have a huge influence on the course of the pandemic. And it’s worth noting that these models are based on strict and widespread social distancing that lasts through May: Staying in shutdown for longer will help ease the burden on the healthcare system, which will save lives. If restrictions ease up in the wrong places too early, cases of the disease could surge all over again.
These predictions also don’t include any secondary (or tertiary) waves, which infectious disease researchers currently think are likely to happen once folks are out in public able to spread COVID-19 once more. It’s impossible to know right now how those later waves will turn out. They could be far less dangerous, since herd immunity will be higher and demands on the healthcare system will likely be lower. But it’s also possible that, like the 1918 flu, the second and third waves could be deadlier (many think the influenza virus developed a new mutation that increased the impact of those waves, but others are skeptical). Until vaccines are ready for general use—which will likely take around a year, if not a bit longer—we must be prepared for future peaks of COVID-19 to be as deadly serious as the initial outbreak.
But while these graphs shouldn’t be taken as a guaranteed predictor of your state’s COVID-19 outcomes, there is one message you can absolutely take away from the data: The important thing right now is to continue to stay home. The sooner we all hunker down, the sooner we’ll be able to come back out again.
Related posts:
 Here’s where all the COVID-19 vaccine candidates currently stand
15 Art Therapy Activities Kids Can Do By Themselves
11 DIY Wall Mural Ideas You Can Paint In A Day
Here’s where all the COVID-19 vaccine candidates currently stand
15 Art Therapy Activities Kids Can Do By Themselves
11 DIY Wall Mural Ideas You Can Paint In A Day
 The Best New Cookbooks for Fall 2019
8 Colorful DIY Sidewalk Chalk Ideas
5 Ways To Boost Your Immune System and Fend off Coronavirus
The Best New Cookbooks for Fall 2019
8 Colorful DIY Sidewalk Chalk Ideas
5 Ways To Boost Your Immune System and Fend off Coronavirus
 The US is officially COVID-19′s epicenter
The US is officially COVID-19′s epicenter
 60 Gifts In A Jar That Are Oh So Cute And Easy To DIY
60 Gifts In A Jar That Are Oh So Cute And Easy To DIY
 How to tell seasonal allergies from COVID-19 symptoms
How to tell seasonal allergies from COVID-19 symptoms
 Coronavirus (COVID-19) Symptoms and Protective Measures to Take
Coronavirus (COVID-19) Symptoms and Protective Measures to Take
 COVID-19 herd immunity isn’t happening any time soon
14 Berry Smoothies You Can Make At Home For A Tropical Treat
16 Easter Recipes To Whip Up For A Tasty At-Home Celebration
COVID-19 herd immunity isn’t happening any time soon
14 Berry Smoothies You Can Make At Home For A Tropical Treat
16 Easter Recipes To Whip Up For A Tasty At-Home Celebration
 Inside the race to develop a safe COVID-19 vaccine
Inside the race to develop a safe COVID-19 vaccine